Calcaneal Apophysitis Facts And Figures
Overview
Sever's Disease (Calcaneal Aphophysitis) is not a disease, but a repetitious strain injury common in children between the ages of 8 and 14 years old. It is a common cause of heel pain, particularly in the very active child. Patients with Sever's disease complain of pain in the bottom surface region of the back of the heel. This is where the growth plate is located, and is not fully developed or calcified in a child's foot.
Causes
Heel pain is very common in children due to the fact they are cnstantly growing. In most children, the heel bone (the calcaneus) is not fully developed until the age of 14 or older. Until then, new bone is forming at the growth plate of the foot (the apophysis, located at the back of the heel), an area which is softer than others due to its role in accommodating the growth. Repetitive stress on the growth plate due to walking, running and sports causes inflammation in the heel area. Because the heel's growth plate is sensitive, repeated running and pounding on hard surfaces can result in pediatric heel pain. Children and adolescents who take part in a lot of sport are especially vulnerable. Over-pronation (fallen arches and rolling inwards of the feet) will increase the impact on the growth plate and is therefore a significant cause and a major contributing factor to heel pain in children.
Symptoms
Pain is usually felt at the back of the heel and around the sides of the heel. If you squeeze the back of the heel from both sides simultaneously and pain is experienced Sever?s disease is more than likely present.
Diagnosis
A doctor can usually tell that a child has Sever's disease based on the symptoms reported. To confirm the diagnosis, the doctor will probably examine the heels and ask about the child's activity level and participation in sports. The doctor might also use the squeeze test, squeezing the back part of the heel from both sides at the same time to see if doing so causes pain. The doctor might also ask the child to stand on tiptoes to see if that position causes pain. Although imaging tests such as X-rays generally are not that helpful in diagnosing Sever's disease, some doctors order them to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
The doctor might recommend that a child with Sever's disease. perform foot and leg exercises to stretch and strengthen the leg muscles and tendons, elevate and apply ice (wrapped in a towel, not applied directly to the skin) to the injured heel for 20 minutes two or three times per day, even on days when the pain is not that bad, to help reduce swelling, use an elastic wrap or compression stocking that is designed to help decrease pain and swelling, take an over-the-counter medicine to reduce pain and swelling, such as acetaminophen (Tylenol) or ibuprofen (Advil, Motrin).
Sever's Disease (Calcaneal Aphophysitis) is not a disease, but a repetitious strain injury common in children between the ages of 8 and 14 years old. It is a common cause of heel pain, particularly in the very active child. Patients with Sever's disease complain of pain in the bottom surface region of the back of the heel. This is where the growth plate is located, and is not fully developed or calcified in a child's foot.
Causes
Heel pain is very common in children due to the fact they are cnstantly growing. In most children, the heel bone (the calcaneus) is not fully developed until the age of 14 or older. Until then, new bone is forming at the growth plate of the foot (the apophysis, located at the back of the heel), an area which is softer than others due to its role in accommodating the growth. Repetitive stress on the growth plate due to walking, running and sports causes inflammation in the heel area. Because the heel's growth plate is sensitive, repeated running and pounding on hard surfaces can result in pediatric heel pain. Children and adolescents who take part in a lot of sport are especially vulnerable. Over-pronation (fallen arches and rolling inwards of the feet) will increase the impact on the growth plate and is therefore a significant cause and a major contributing factor to heel pain in children.
Symptoms
Pain is usually felt at the back of the heel and around the sides of the heel. If you squeeze the back of the heel from both sides simultaneously and pain is experienced Sever?s disease is more than likely present.
Diagnosis
A doctor can usually tell that a child has Sever's disease based on the symptoms reported. To confirm the diagnosis, the doctor will probably examine the heels and ask about the child's activity level and participation in sports. The doctor might also use the squeeze test, squeezing the back part of the heel from both sides at the same time to see if doing so causes pain. The doctor might also ask the child to stand on tiptoes to see if that position causes pain. Although imaging tests such as X-rays generally are not that helpful in diagnosing Sever's disease, some doctors order them to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
The doctor might recommend that a child with Sever's disease. perform foot and leg exercises to stretch and strengthen the leg muscles and tendons, elevate and apply ice (wrapped in a towel, not applied directly to the skin) to the injured heel for 20 minutes two or three times per day, even on days when the pain is not that bad, to help reduce swelling, use an elastic wrap or compression stocking that is designed to help decrease pain and swelling, take an over-the-counter medicine to reduce pain and swelling, such as acetaminophen (Tylenol) or ibuprofen (Advil, Motrin).
What Are The Major Causes Of Posterior Tibial Tendon Dysfunction (PTTD) ?
Overview
Another common term for this condition is Posterior Tibial Tendon Dysfunction (PTTD). There is a cause-effect relationship between pronation, flatfoot deformity and subsequent tenosynovitis of the posterior tibial tendon. Mechanical irritation of the tendon may lead to synovitis, partial tearing and eventually full rupture of the tendon. Other structures, including ligaments and the plantar fascia, have also been shown to contribute to the arch collapsing. As the deformity progresses, these structures have been shown to attenuate and rupture as well. In later stages, subluxation of various joints lead to a valgus rearfoot and transverse plane deformity of the forefoot. These deformities can become fixed and irreducible as significant osteoarthritis sets in. 
Causes
Several risk factors are associated with PTT dysfunction, including high blood pressure, obesity, diabetes, previous ankle surgery or trauma and exposure to steroids. A person who suspects that they are suffering from PTT dysfunction should seek medical attention earlier rather than later. It is much easier to treat early and avoid a collapsed arch than it is to repair one. When the pain first happens and there is no significant flatfoot deformity, initial treatments include rest, oral anti-inflammatory medications and, depending on the severity, a special boot or brace.
Symptoms
Pain and swelling behind the inside of your ankle and along your instep. You may be tender behind the inner ankle where the posterior tibial tendon courses and occasionally get burning, shooting, tingling or stabbing pain as a result of inflammation of the nerve inside the tarsal tunnel. Difficulty walking, the inability to walk long distances and a generalised ache while walking even short distances. This may probably become more pronounced at the end of each day. Change in foot shape, sometimes your tendon stretches out, this is due to weakening of the tendon and ligaments. When this occurs, the arch in your foot flattens and a flatfoot deformity occurs, presenting a change in foot shape. Inability to tip-toe, a way of diagnosing Posterior Tibial Tendon Dysfunction is difficulty or inability to ?heel rise? (stand on your toes on one foot). Your tibialis posterior tendon enables you to perform this manoeuvre effectively. You may also experience pain upon attempting to perform a heel rise.
Diagnosis
It is of great importance to have a full evaluation, by a foot and ankle specialist with expertise in addressing complex flatfoot deformities. No two flat feet are alike; therefore, "Universal" treatment plans do not exist for the Adult Flatfoot. It is important to have a custom treatment plan that is tailored to your specific foot. That starts by first understanding all the intricacies of your foot, through an extensive evaluation. X-rays of the foot and ankle are standard, and MRI may be used to better assess the quality of the PT Tendon.
Non surgical Treatment
Because of the progressive nature of PTTD, early treatment is advised. If treated early enough, your symptoms may resolve without the need for surgery and progression of your condition can be arrested. In contrast, untreated PTTD could leave you with an extremely flat foot, painful arthritis in the foot and ankle, and increasing limitations on walking, running, or other activities. In many cases of PTTD, treatment can begin with non-surgical approaches that may include. Orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may provide you with an ankle brace or a custom orthotic device that fits into the shoe. Immobilization. Sometimes a short-leg cast or boot is worn to immobilize the foot and allow the tendon to heal, or you may need to completely avoid all weight-bearing for a while. Physical therapy. Ultrasound therapy and exercises may help rehabilitate the tendon and muscle following immobilization. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Shoe modifications. Your foot and ankle surgeon may advise changes to make with your shoes and may provide special inserts designed to improve arch support. 
Surgical Treatment
Surgical correction is dependent on the severity of symptoms and the stage of deformity. The goals of surgery are to create a more functional and stable foot. There are multiple procedures available to the surgeon and it may take several to correct a flatfoot deformity. Usually surgical treatment begins with removal of inflammatory tissue and repair of the posterior tibial tendon. A tendon transfer is performed if the posterior tibial muscle is weak or the tendon is badly damaged. The most commonly used tendon is the flexor digitorum longus tendon. This tendon flexes or moves the lesser toes downward. The flexor digitorum longus tendon is utilized due to its close proximity to the posterior tibial tendon and because there are minimal side effects with its loss. The remainder of the tendon is sutured to the flexor hallucis longus tendon that flexes the big toe so that little function is loss.
The Reality About Adult Aquired Flat Feet
Overview
Posterior tibial tendon insufficiency (also called posterior tibial tendon dysfunction or adult acquired flatfoot) has been named literally after failure of the posterior tibial tendon. However, the condition is caused not only by the progressive failure of the posterior tibial tendon; it is also failure of associated ligaments and joints on the inner side of the ankle and foot. This results in collapse of the arch of the foot, along with the deformity which most often becomes the debilitating problem in its later stages. While at the beginning the common symptom is pain over the tendon in the inner part of the hindfoot and midfoot, later on it is the deformity that can threaten a person's ability to walk. Just as the tendon degenerates and loses its function, other soft tissue on the same inner side of the foot - namely the ligaments - degenerate and fail. Ligaments are responsible for holding bones in place, and when they fail, bones shift to places where they shouldn?t; deformity is the result. The deformity causes malalignment, leading to more stress and failure of the ligaments.
Causes
Flat footedness, most people who develop the condition already have flat feet. With overuse or continuous loading, a change occurs where the arch begins to flatten more than before, with pain and swelling developing on the inside of the ankle. Inadequate support from footwear may occasionally be a contributing factor. Trauma or injury, occasionally this condition may be due to fracture, sprain or direct blow to the tendon. Age, the risk of developing Posterior Tibial Tendon Dysfunction increases with age and research has suggested that middle aged women are more commonly affected. Other possible contributing factors - being overweight and inflammatory arthritis.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
Looking at the patient when they stand will usually demonstrate a flatfoot deformity (marked flattening of the medial longitudinal arch). The front part of the foot (forefoot) is often splayed out to the side. This leads to the presence of a ?too many toes? sign. This sign is present when the toes can be seen from directly behind the patient. The gait is often somewhat flatfooted as the patient has the dysfunctional posterior tibial tendon can no longer stabilize the arch of the foot. The physician?s touch will often demonstrate tenderness and sometimes swelling over the inside of the ankle just below the bony prominence (the medial malleolus). There may also be pain in the outside aspect of the ankle. This pain originates from impingement or compression of two tendons between the outside ankle bone (fibula) and the heel bone (calcaneus) when the patient is standing.
Non surgical Treatment
Treatment will vary depending on the degree of your symptoms. Generally, we would use a combination of rest, immobilization, orthotics, braces, and physical therapy to start. The goal is to keep swelling and inflammation under control and limit the stress on the tendon while it heals. Avoidance of activities that stress the tendon will be necessary. Once the tendon heals and you resume activity, physical therapy will further strengthen the injured tendon and help restore flexibility. Surgery may be necessary if the tendon is torn or does not respond to these conservative treatment methods. Your posterior tibial tendon is vital for normal walking. When it is injured in any way, you risk losing independence and mobility. Keep your foot health a top priority and address any pain or problems quickly. Even minor symptoms could progress into chronic problems, so don?t ignore your foot pain.

Surgical Treatment
For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.
Posterior tibial tendon insufficiency (also called posterior tibial tendon dysfunction or adult acquired flatfoot) has been named literally after failure of the posterior tibial tendon. However, the condition is caused not only by the progressive failure of the posterior tibial tendon; it is also failure of associated ligaments and joints on the inner side of the ankle and foot. This results in collapse of the arch of the foot, along with the deformity which most often becomes the debilitating problem in its later stages. While at the beginning the common symptom is pain over the tendon in the inner part of the hindfoot and midfoot, later on it is the deformity that can threaten a person's ability to walk. Just as the tendon degenerates and loses its function, other soft tissue on the same inner side of the foot - namely the ligaments - degenerate and fail. Ligaments are responsible for holding bones in place, and when they fail, bones shift to places where they shouldn?t; deformity is the result. The deformity causes malalignment, leading to more stress and failure of the ligaments.
Causes
Flat footedness, most people who develop the condition already have flat feet. With overuse or continuous loading, a change occurs where the arch begins to flatten more than before, with pain and swelling developing on the inside of the ankle. Inadequate support from footwear may occasionally be a contributing factor. Trauma or injury, occasionally this condition may be due to fracture, sprain or direct blow to the tendon. Age, the risk of developing Posterior Tibial Tendon Dysfunction increases with age and research has suggested that middle aged women are more commonly affected. Other possible contributing factors - being overweight and inflammatory arthritis.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
Looking at the patient when they stand will usually demonstrate a flatfoot deformity (marked flattening of the medial longitudinal arch). The front part of the foot (forefoot) is often splayed out to the side. This leads to the presence of a ?too many toes? sign. This sign is present when the toes can be seen from directly behind the patient. The gait is often somewhat flatfooted as the patient has the dysfunctional posterior tibial tendon can no longer stabilize the arch of the foot. The physician?s touch will often demonstrate tenderness and sometimes swelling over the inside of the ankle just below the bony prominence (the medial malleolus). There may also be pain in the outside aspect of the ankle. This pain originates from impingement or compression of two tendons between the outside ankle bone (fibula) and the heel bone (calcaneus) when the patient is standing.
Non surgical Treatment
Treatment will vary depending on the degree of your symptoms. Generally, we would use a combination of rest, immobilization, orthotics, braces, and physical therapy to start. The goal is to keep swelling and inflammation under control and limit the stress on the tendon while it heals. Avoidance of activities that stress the tendon will be necessary. Once the tendon heals and you resume activity, physical therapy will further strengthen the injured tendon and help restore flexibility. Surgery may be necessary if the tendon is torn or does not respond to these conservative treatment methods. Your posterior tibial tendon is vital for normal walking. When it is injured in any way, you risk losing independence and mobility. Keep your foot health a top priority and address any pain or problems quickly. Even minor symptoms could progress into chronic problems, so don?t ignore your foot pain.
Surgical Treatment
For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.
Coping With Achilles Tendinitis
Overview
 Achilles tendinitis is an overuse injury of the Achilles tendon, the band of tissue that connects calf muscles at the back of the lower leg to your heel bone. Achilles tendinitis most commonly occurs in runners who have suddenly increased the intensity or duration of their runs. It's also common in middle-aged people who play sports, such as tennis or basketball, only on the weekends. Most cases of Achilles tendinitis can be treated with relatively simple, at-home care under your doctor's supervision. Self-care strategies are usually necessary to prevent recurring episodes. More-serious cases of Achilles tendinitis can lead to tendon tears (ruptures) that may require surgical repair.
Achilles tendinitis is an overuse injury of the Achilles tendon, the band of tissue that connects calf muscles at the back of the lower leg to your heel bone. Achilles tendinitis most commonly occurs in runners who have suddenly increased the intensity or duration of their runs. It's also common in middle-aged people who play sports, such as tennis or basketball, only on the weekends. Most cases of Achilles tendinitis can be treated with relatively simple, at-home care under your doctor's supervision. Self-care strategies are usually necessary to prevent recurring episodes. More-serious cases of Achilles tendinitis can lead to tendon tears (ruptures) that may require surgical repair.
Causes
The calf is under a lot of strain when running: it is not only put on stretch during landing of the foot, but it also has to produce the tension needed to support body weight and absorb the shock of landing. This is what is called an ?eccentric load?. Excessive eccentric loading - either by way of a dramatic increase in mileage, or excessive hill running, or faulty running posture - could very well be the cause of a runner?s achilles tendinitis. The calf strain translates downward into the achilles tendon where it attaches to the heel, and inflammation ensues. Inflammation then causes scarring and fibrosis of tissues, which in turn inflicts pain upon stretching or use. Risk factors for Achilles tendinitis also include spending prolonged amounts of time standing or walking.
Symptoms
Common symptoms of Achilles tendinitis include weakness in the leg, slight pain above the heel in the lower leg after activity, feeling of stiffness in the leg that usually appears in the morning and lessens throughout the day, bad pain the day after exercising, pain as you climb stairs or go uphill, swelling in the area of the Achilles tendon, creaking or cracking noise when you press on the Achilles tendon.
Diagnosis
In diagnosing Achilles tendonitis or tendonosis, the surgeon will examine the patient?s foot and ankle and evaluate the range of motion and condition of the tendon. The extent of the condition can be further assessed with x-rays or other imaging modalities.
Nonsurgical Treatment
Physical therapy is the first and most useful defense for achilles tendonitis because of the two presentations outlined above. Treatments for the two types are quite different in approach. Midsubstance tendinitis responds well to stretching, whereas insertional tendnitis tends to be aggravated more by it. Depend on your trusted physical therapist to differentiate between the two and follow their guidelines on exercises and running modifications. Running gait patterns that show excessive ?sinking postures? tend to point to the source of achilles tendon problems. Altering your gait in the midstance phase of the cycle can reduce the load on the tendon dramatically and thereby reduce pain. Rely on your running physical therapist for proper guidance on altering your gait the right way. Stride Strong?s Portland Running Clinic gait analysis can identify and fix potential issues before pain sets in. Icing at the onset of acute achilles pain (i.e. when the injury is fresh and new) would help control the inflammation. Your next step should be to call our number for an appointment.
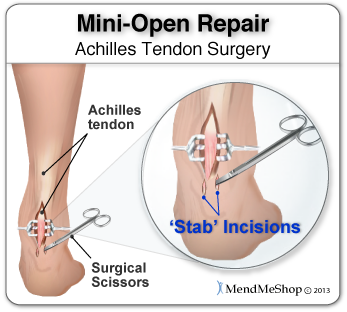
Surgical Treatment
Many people don't realize that Achilles tendon surgery can be very traumatic to your body. The type of trauma you experience after surgery can be compared to what you go through when you first injured your Achilles tendon. During the first 24 to 72 hours after the surgery your ankle will be tender, swollen and very painful. Your leg will be weak and unstable making it impossible for you to put weight on your leg without some kind of help. This is why your doctor or surgeon will have you outfitted for a cast, ankle brace and/or crutches before the procedure. When you are relying on a cast/brace and crutches your Achilles tendon is less likely to be as active as it once was. This is usually why atrophy (loss) of your lower leg muscles (specifically your calf muscle) happens. In general, more than 80%* of people who undergo surgery for an injured Achilles Tendon are able to return to their active lifestyle. In order to avoid re-injury, it is important to commit to a regular conservative therapy routine.
Prevention
A 2014 study looked at the effect of using foot orthotics on the Achilles tendon. The researchers found that running with foot orthotics resulted in a significant decrease in Achilles tendon load compared to running without orthotics. This study indicates that foot orthoses may act to reduce the incidence of chronic Achilles tendon pathologies in runners by reducing stress on the Achilles tendon1. Orthotics seem to reduce load on the Achilles tendon by reducing excessive pronation,
Achilles tendinitis is an overuse injury of the Achilles tendon, the band of tissue that connects calf muscles at the back of the lower leg to your heel bone. Achilles tendinitis most commonly occurs in runners who have suddenly increased the intensity or duration of their runs. It's also common in middle-aged people who play sports, such as tennis or basketball, only on the weekends. Most cases of Achilles tendinitis can be treated with relatively simple, at-home care under your doctor's supervision. Self-care strategies are usually necessary to prevent recurring episodes. More-serious cases of Achilles tendinitis can lead to tendon tears (ruptures) that may require surgical repair.
Causes
The calf is under a lot of strain when running: it is not only put on stretch during landing of the foot, but it also has to produce the tension needed to support body weight and absorb the shock of landing. This is what is called an ?eccentric load?. Excessive eccentric loading - either by way of a dramatic increase in mileage, or excessive hill running, or faulty running posture - could very well be the cause of a runner?s achilles tendinitis. The calf strain translates downward into the achilles tendon where it attaches to the heel, and inflammation ensues. Inflammation then causes scarring and fibrosis of tissues, which in turn inflicts pain upon stretching or use. Risk factors for Achilles tendinitis also include spending prolonged amounts of time standing or walking.
Symptoms
Common symptoms of Achilles tendinitis include weakness in the leg, slight pain above the heel in the lower leg after activity, feeling of stiffness in the leg that usually appears in the morning and lessens throughout the day, bad pain the day after exercising, pain as you climb stairs or go uphill, swelling in the area of the Achilles tendon, creaking or cracking noise when you press on the Achilles tendon.
Diagnosis
In diagnosing Achilles tendonitis or tendonosis, the surgeon will examine the patient?s foot and ankle and evaluate the range of motion and condition of the tendon. The extent of the condition can be further assessed with x-rays or other imaging modalities.
Nonsurgical Treatment
Physical therapy is the first and most useful defense for achilles tendonitis because of the two presentations outlined above. Treatments for the two types are quite different in approach. Midsubstance tendinitis responds well to stretching, whereas insertional tendnitis tends to be aggravated more by it. Depend on your trusted physical therapist to differentiate between the two and follow their guidelines on exercises and running modifications. Running gait patterns that show excessive ?sinking postures? tend to point to the source of achilles tendon problems. Altering your gait in the midstance phase of the cycle can reduce the load on the tendon dramatically and thereby reduce pain. Rely on your running physical therapist for proper guidance on altering your gait the right way. Stride Strong?s Portland Running Clinic gait analysis can identify and fix potential issues before pain sets in. Icing at the onset of acute achilles pain (i.e. when the injury is fresh and new) would help control the inflammation. Your next step should be to call our number for an appointment.
Surgical Treatment
Many people don't realize that Achilles tendon surgery can be very traumatic to your body. The type of trauma you experience after surgery can be compared to what you go through when you first injured your Achilles tendon. During the first 24 to 72 hours after the surgery your ankle will be tender, swollen and very painful. Your leg will be weak and unstable making it impossible for you to put weight on your leg without some kind of help. This is why your doctor or surgeon will have you outfitted for a cast, ankle brace and/or crutches before the procedure. When you are relying on a cast/brace and crutches your Achilles tendon is less likely to be as active as it once was. This is usually why atrophy (loss) of your lower leg muscles (specifically your calf muscle) happens. In general, more than 80%* of people who undergo surgery for an injured Achilles Tendon are able to return to their active lifestyle. In order to avoid re-injury, it is important to commit to a regular conservative therapy routine.
Prevention
A 2014 study looked at the effect of using foot orthotics on the Achilles tendon. The researchers found that running with foot orthotics resulted in a significant decrease in Achilles tendon load compared to running without orthotics. This study indicates that foot orthoses may act to reduce the incidence of chronic Achilles tendon pathologies in runners by reducing stress on the Achilles tendon1. Orthotics seem to reduce load on the Achilles tendon by reducing excessive pronation,
Complications Caused By Diabetic Feet
Persistent unilateral (one -sided) swelling of feet can be a sign of serious damage to the bones and joints of his feet and needs to be shown to a doctor immediately. If the foot wear is worn out at particular place, it is indicative of extra pressure being applied at that area of the foot and needs to be shown to the doctor at the earliest. While traveling, one must not remove his/her footwear and rest the feet on the floor of the vehicle. No amount of drugs/medicines can keep a patient's feet intact unless the patient is wearing properly designed footwear. All foot wear must always be worn with socks. It is necessary to avoid direct contact between the footwear and skin. Socks also help in reducing the damage to the skin of the fore foot. The heel of the foot should be completely supported by FULL HEEL COUNTER. Diabetic neuroischemic foot.

We understand that prevention needs to be a combination of systemic disease control and self foot-care, which includes proper foot hygiene, foot inspection and proper foot gear. As health care professionals, we are at a loss for effective methods to influence behaviors in our patients, especially because behaviors are difficult to address in the short period of time we have with them. Apparently intelligence has little to do with an inability to care for one's self, as many high functioning adults may have rather questionable personal habits. The study looked at 302 type II diabetics from the VA healthcare system in Taiwan divided into two groups; 155 received group lectures in addition to routine healthcare, and 147 received only routine care. A retrospective review of medical records and a structured interview were conducted to determine the foot care quality among the two groups. Epidemiology and prevention.
There is the specific broken ankle recovery occasion any particular one should know. This really is to help no cost your ex in the popular broken ankle recovery oversight that will other folks happen to be doing. Eventhough it can be simple to comprehend that you could really hope his or her foot to mend quick, she must likewise agree to the reality that broken ankle recovery moment probably won't match their preference.
Diabetic foot ulcers as one of the most common complications of diabetes mellitus are defined as nonhealing or long-lasting chronic skin ulcers in diabetic patients. Low level laser therapy (LLLT) on wound areas as well as on acupuncture points, as a noninvasive, pain-free method with minor side effects, has been considered as a possible treatment option for the diabetic foot syndrome. The majority of clinical studies show a potential benefit of LLLT in wound healing of diabetic ulcers.
Under normal circumstances, a blister created in this manner wouldn't present a health risk, but diabetics have poor circulation, putting them in danger of infection complications. The American Diabetes Association lists the infection as the fungal contagion most often found in those with diabetes. Candida albicans presents an itchy, red rash surrounded by blisters and scales that occur in warm, moist folds of skin - such as the area under breasts, between the fingers and toes, under the foreskin, in the armpits and groin. Prescription medication treats the fungal infection in diabetics, effectively clearing up the blisters.
Dyshidrotic eczema, which is also called vesicular eczema of hands or feet, is a form of eczema that is characterized by cracked skin and itchy blisters. The affected individual Foot Conditions must refrain from scratching over the affected skin. Psoriasis is a skin condition that is characterized by the development of inflamed patches of skin and silvery scales.
We understand that prevention needs to be a combination of systemic disease control and self foot-care, which includes proper foot hygiene, foot inspection and proper foot gear. As health care professionals, we are at a loss for effective methods to influence behaviors in our patients, especially because behaviors are difficult to address in the short period of time we have with them. Apparently intelligence has little to do with an inability to care for one's self, as many high functioning adults may have rather questionable personal habits. The study looked at 302 type II diabetics from the VA healthcare system in Taiwan divided into two groups; 155 received group lectures in addition to routine healthcare, and 147 received only routine care. A retrospective review of medical records and a structured interview were conducted to determine the foot care quality among the two groups. Epidemiology and prevention.
There is the specific broken ankle recovery occasion any particular one should know. This really is to help no cost your ex in the popular broken ankle recovery oversight that will other folks happen to be doing. Eventhough it can be simple to comprehend that you could really hope his or her foot to mend quick, she must likewise agree to the reality that broken ankle recovery moment probably won't match their preference.
Diabetic foot ulcers as one of the most common complications of diabetes mellitus are defined as nonhealing or long-lasting chronic skin ulcers in diabetic patients. Low level laser therapy (LLLT) on wound areas as well as on acupuncture points, as a noninvasive, pain-free method with minor side effects, has been considered as a possible treatment option for the diabetic foot syndrome. The majority of clinical studies show a potential benefit of LLLT in wound healing of diabetic ulcers.
Under normal circumstances, a blister created in this manner wouldn't present a health risk, but diabetics have poor circulation, putting them in danger of infection complications. The American Diabetes Association lists the infection as the fungal contagion most often found in those with diabetes. Candida albicans presents an itchy, red rash surrounded by blisters and scales that occur in warm, moist folds of skin - such as the area under breasts, between the fingers and toes, under the foreskin, in the armpits and groin. Prescription medication treats the fungal infection in diabetics, effectively clearing up the blisters.
Dyshidrotic eczema, which is also called vesicular eczema of hands or feet, is a form of eczema that is characterized by cracked skin and itchy blisters. The affected individual Foot Conditions must refrain from scratching over the affected skin. Psoriasis is a skin condition that is characterized by the development of inflamed patches of skin and silvery scales.
What Brings About Plantar Fasciitis And The Ways To Cure It

Overview
The plantar fascia (a connective tissue structure) stretches from the toes and ball of the foot, through the arch, and connects to the heel bone in three places: outside, center and inside. Normally it helps the foot spring as it rolls forward. It also provides support for the arch of the foot. The plantar fascia helps keep the foot on track, cutting down on oscillation. When the foot over-pronates (rolls to the inside) the plantar fascia tries to stabilize it and prevent excessive roll. In time, the inside and sometimes center connections are overstressed and pull away from their attachments. The first sign is usually heel pain as you rise in the morning. When you walk around, the pain may subside, only to return the next morning. Inflammation and increased soreness are the results of long-term neglect and continued abuse. A heel bone spur may develop after a long period of injury when there is no support for the heel. The plantar fascia attaches to the heel bone with small fibers. When these become irritated they become inflamed with blood containing white blood cells. Within the white blood cells are osteoblasts which calcify to form bone spurs and calcium deposits. The body is trying to reduce stress on that area by building a bone in the direction of stress. Unfortunately, these foreign substances cause pain and further irritation in the surrounding soft tissue.
Causes
Plantar fasciitis generally occurs over time, rather than being the result of a single event. Micro trauma from repetitive stress to the tissue often combines with a biomechanical deficiency of the foot to produce the condition. In addition, arthritic and metabolic factors may contribute to the development of this injury, (though they are unlikely to affect young athletes). A variety of training errors commonly lead to plantar fasciitis, particularly a rapid increase in either volume or intensity of athletic activity. Volume refers to the distance or time an athlete performs, while intensity refers to the pace of activity and/or the recovery time allowed following performance.
Symptoms
The most common symptom is pain and stiffness in the bottom of the heel. The heel pain may be dull or sharp. The bottom of the foot may also ache or burn. The pain is often worse in the morning when you take your first steps, after standing or sitting for awhile, when climbing stairs, after intense activity. The pain may develop slowly over time, or come on suddenly after intense activity.
Diagnosis
X-rays are a commonly used diagnostic imaging technique to rule out the possibility of a bone spur as a cause of your heel pain. A bone spur, if it is present in this location, is probably not the cause of your pain, but it is evidence that your plantar fascia has been exerting excessive force on your heel bone. X-ray images can also help determine if you have arthritis or whether other, more rare problems, stress fractures, bone tumors-are contributing to your heel pain.
Non Surgical Treatment
Treatment initially involves offloading the plantar fascia by aoiding aggravating factors, such as running. Taping, this can work very well to alleviate pain, and can be almost immediate. It isn't a long-term solution, but can relieve symptoms in the beginning. Using a night splint to stretch the calf, so that less load is placed on the plantar fascia (if tightness in the calf is a factor). Using a gel heel cup, this can act to increase shock absorption, and by raising the heel there is also less stretch on the calf. So, temporarily, this may relieve pain in someone who has a tight calf. Massage, but this depends if the plantarfascia is actually tight or just painful. If it is tight, then massage can temporarily relieve the pain, but if it is irritated then taping and corrective footwear is preferable.

Surgical Treatment
Most practitioners agree that treatment for plantar fasciitis is a slow process. Most cases resolve within a year. If these more conservative measures don't provide relief after this time, your doctor may suggest other treatment. In such cases, or if your heel pain is truly debilitating and interfering with normal activity, your doctor may discuss surgical options with you. The most common surgery for plantar fasciitis is called a plantar fascia release and involves releasing a portion of the plantar fascia from the heel bone. A plantar fascia release can be performed through a regular incision or as endoscopic surgery, where a tiny incision allows a miniature scope to be inserted and surgery to be performed. About one in 20 patients with plantar fasciitis will need surgery. As with any surgery, there is still some chance that you will continue to have pain afterwards.
Stretching Exercises
The following exercises are commonly prescribed to patients with this condition. You should discuss the suitability of these exercises with your physiotherapist prior to beginning them. Generally, they should be performed 2 - 3 times daily and only provided they do not cause or increase symptoms. Your physiotherapist can advise when it is appropriate to begin the initial exercises and eventually progress to the intermediate and advanced exercises. As a general rule, addition of exercises or progression to more advanced exercises should take place provided there is no increase in symptoms. Calf Stretch with Towel. Begin this stretch in long sitting with your leg to be stretched in front of you. Your knee and back should be straight and a towel or rigid band placed around your foot as demonstrated. Using your foot, ankle and the towel, bring your toes towards your head until you feel a stretch in the back of your calf, Achilles tendon, plantar fascia or leg. Hold for 5 seconds and repeat 10 times at a mild to moderate stretch provided the exercise is pain free. Resistance Band Calf Strengthening. Begin this exercise with a resistance band around your foot as demonstrated and your foot and ankle held up towards your head. Slowly move your foot and ankle down against the resistance band as far as possible and comfortable without pain, tightening your calf muscle. Very slowly return back to the starting position. Repeat 10 - 20 times provided the exercise is pain free.
What Is Heel Pain
5I1dimw~~60_35.JPG)
Overview
Plantar fasciitis is the most common cause of heel pain. The plantar fascia is the flat band of tissue (ligament) that connects your heel bone to your toes. It supports the arch of your foot. If you strain your plantar fascia, it gets weak, swollen, and irritated (inflamed). Then your heel or the bottom of your foot hurts when you stand or walk. Plantar fasciitis is common in middle-aged people. It also occurs in younger people who are on their feet a lot, like athletes or soldiers. It can happen in one foot or both feet.
Causes
Plantar fasciitis is caused by straining the ligament that supports your arch. Repeated strain can cause tiny tears in the ligament. These can lead to pain and swelling. This is more likely to happen if your feet roll inward too much when you walk ( excessive pronation ). You have high arches or flat feet. You walk, stand, or run for long periods of time, especially on hard surfaces. You are overweight. You wear shoes that don't fit well or are worn out. You have tight Achilles tendons or calf muscles.
Symptoms
A sharp pain in the center of your heel will most likely be one of the biggest symptoms of plantar fasciitis. A classic sign of plantar fasciitis is when the pain is worst during the first steps you take in the morning.
Diagnosis
Plantar fasciosis is confirmed if firm thumb pressure applied to the calcaneus when the foot is dorsiflexed elicits pain. Fascial pain along the plantar medial border of the fascia may also be present. If findings are equivocal, demonstration of a heel spur on x-ray may support the diagnosis; however, absence does not rule out the diagnosis, and visible spurs are not generally the cause of symptoms. Also, infrequently, calcaneal spurs appear ill defined on x-ray, exhibiting fluffy new bone formation, suggesting spondyloarthropathy (eg, ankylosing spondylitis, reactive arthritis. If an acute fascial tear is suspected, MRI is done.
Non Surgical Treatment
A doctor may prescribe anti-inflammatory medication such as ibuprofen to help reduce pain and inflammation. Electrotherapy such as ultrasound or laser may also help with symptoms. An X-ray may be taken to see if there is any bone growth or calcification, known as a heel spur but this is not necessarily a cause of pain. Deep tissue sports massage techniques can reduce the tension in and stretch the plantar fascia and the calf muscles. Extracorporeal shock wave therapy has been known to be successful and a corticosteroid injection is also an option.

Surgical Treatment
Plantar fasciotomy is often considered after conservative treatment has failed to resolve the issue after six months and is viewed as a last resort. Minimally invasive and endoscopic approaches to plantar fasciotomy exist but require a specialist who is familiar with certain equipment. Heel spur removal during plantar fasciotomy has not been found to improve the surgical outcome. Plantar heel pain may occur for multiple reasons and release of the lateral plantar nerve branch may be performed alongside the plantar fasciotomy in select cases. Possible complications of plantar fasciotomy include nerve injury, instability of the medial longitudinal arch of the foot, fracture of the calcaneus, prolonged recovery time, infection, rupture of the plantar fascia, and failure to improve the pain. Coblation (TOPAZ) surgery has recently been proposed as alternative surgical approaches for the treatment of recalcitrant plantar fasciitis.